
Charlie Kirk’s video listing reasons to oppose COVID-19 vaccines contains multiple incorrect, misleading, and unsupported statements


Inadequate support: Reports in the U.S. VAERS database and anecdotes don’t demonstrate that the vaccine caused an adverse event and therefore can’t be used as evidence that a vaccine is unsafe.
Incorrect: Choosing not to vaccinate has consequences for others because it places oneself and others at a higher risk of infection and severe disease, and this increases the spread of the virus within the community.
FULL CLAIM: COVID-19 vaccines were “rushed into market”; VAERS shows an “unusual spike in vaccine adverse events, in myocarditis, in heart-related issues”; “I don’t need to go vaccinate other people to prevent me of getting something the vaccine is supposed to prevent”
REVIEW
On 4 October 2022, American radio host Charlie Kirk posted a video on Facebook titled “Exposing What the Media Won’t Tell You About COVID Vaxx Side Effects”. The video received more than 32,000 views and 3,400 interactions. In it, Kirk named three reasons why he was “against” COVID-19 vaccines but not against other childhood vaccines recommended by the U.S. Centers for Disease Control and Prevention (CDC), like for example the measles, mumps, and rubella (MMR) vaccine.
Kirk’s reasons were that COVID-19 vaccines (1) were developed too fast, (2) are unlikely to be approved for religious exemptions compared to other vaccines, and (3) are associated with more adverse events than other vaccines. To support these arguments, Kirk rehashed several incorrect, misleading, and unsupported claims that fact-checkers debunked before. Below, we review each of these claims.
Claim 1 (Misleading):
“[COVID-19] vaccine, by all independent metrics, was rushed into market”; “it was not given the same sort of trial, the same sort of independent testing” compared to other vaccines
COVID-19 vaccines were indeed developed at a record speed, beating the previous fastest vaccine development in history, which was four years for the mumps vaccine. The argument that COVID-19 vaccines were developed “too fast” has often been used to cast doubts about their safety. However, it is false that this rapid development is because vaccine developers and regulatory agencies cut corners in safety and efficacy testing as Kirk claimed.
Before receiving emergency use authorization (EUA), the COVID-19 vaccines went through the same degree of safety and efficacy testing as would be expected of any vaccine (see Figure 1). First, the vaccine candidates were tested in cells (in vitro) and in experimental animals (in vivo) to assess that they triggered an immune response and protected from the virus[1-5].
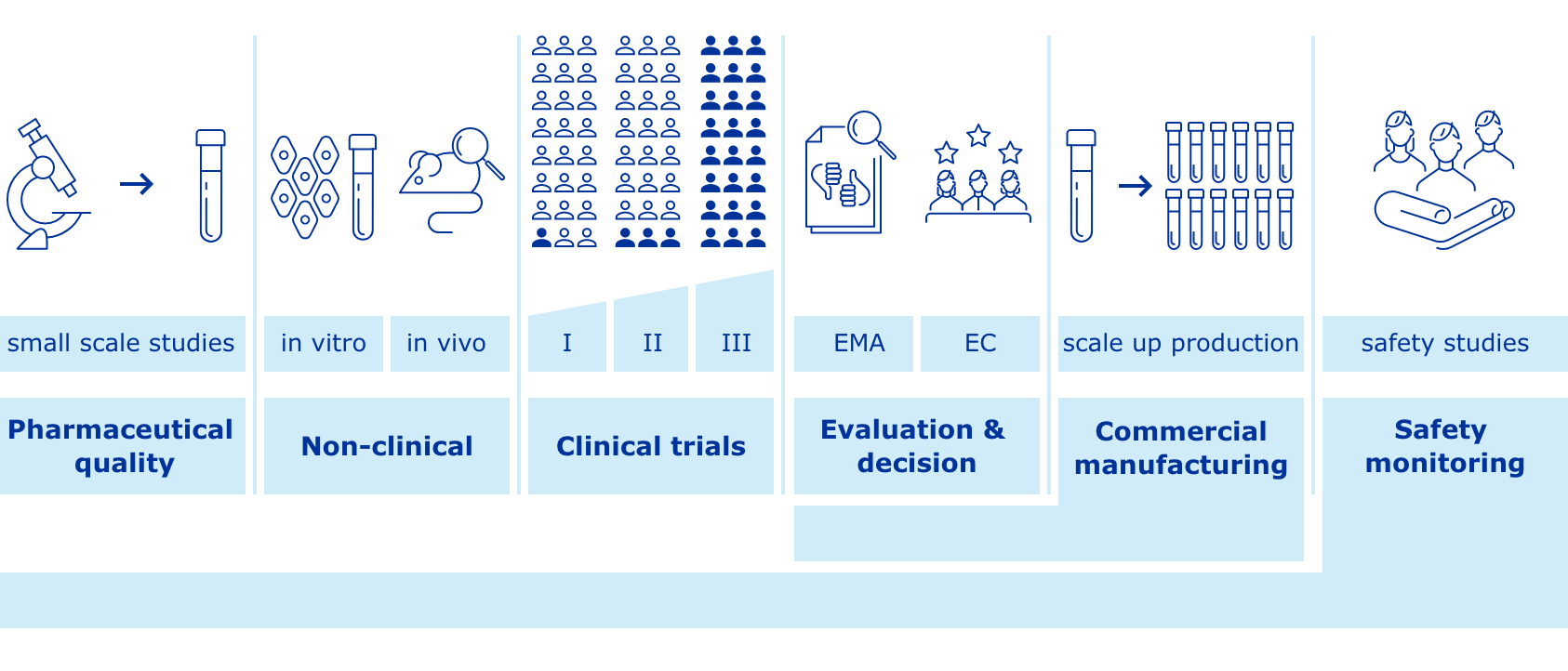
Figure 1. The different stages of vaccine development, including non-clinical studies in the laboratory, clinical trials in volunteers, and post-marketing surveillance. Source: European Medicines Agency.
Then, the safety and efficacy of vaccine candidates were tested in human volunteers in three phases of clinical trials, each one with a larger number of participants[6-8]. Each of these clinical stages had to meet the rigorous requirements of the U.S. Food and Drug Administration.
Finally, COVID-19 vaccines continued to be monitored through several post-marketing surveillance programs that allow regulatory agencies to assess the safety of the vaccines even after they have reached the market.
The fact that previous vaccines took longer to develop doesn’t make them safer than COVID-19 vaccines because the rapid development of COVID-19 vaccines was due to reasons that didn’t compromise their safety, as Health Feedback explained in an earlier review. These reasons included scientific advancements, unprecedented resources, and less bureaucratic obstruction, which made it possible to obtain results faster than usual.
For example, previous knowledge about other coronaviruses similar to SARS-CoV-2 and a better understanding of the immune response allowed scientists to rapidly identify the spike protein of the virus as an effective target for vaccination. The advances in vaccine technology made it possible to use mRNA technology, which is a faster approach than traditional vaccines. The high level of infections worldwide also provided a number of infections in clinical trials that was soon sufficient to estimate the efficacy of the vaccines.
In addition, the exceptional circumstances of the COVID-19 pandemic reduced or eliminated many common limitations in vaccine development, including funding, recruitment of volunteers for clinical trials, cooperation, and bureaucratic red tape, which can delay vaccine development and approval for years.
Claim 2 (Unsupported and Misleading):
VAERS shows an “unusual spike in vaccine adverse events, in myocarditis, in heart-related issues”
Kirk’s claim that COVID-19 vaccines have caused more adverse events than other vaccines is unsupported and misleading because it is based on data from the U.S. Vaccine Adverse Events Reporting System (VAERS), which can’t demonstrate that the vaccine caused the adverse event.
VAERS is a safety monitoring system that collects information about any medical condition (adverse event) that happens following vaccination. But the fact that an adverse event ocurred after receiving a vaccine is necessary but insufficient to demonstrate that the vaccine was responsible for it. To establish a causal link between the vaccine and the adverse event requires further investigations, as Health Feedback explained in an Insight article.
While VAERS serves as an “early warning system” to detect possible safety problems in U.S.-licensed vaccines, VAERS reports alone can’t be used to suggest that a vaccine is unsafe, or to make inferences about its safety compared to other vaccines, as Kirk does. Yet, VAERS reports have been repeatedly misused to imply that COVID-19 vaccines are unsafe, even though the website clearly warns users about its limitations:
“VAERS reports alone generally cannot be used to determine if a vaccine caused or contributed to an adverse event or illness. Some reports may contain information that is incomplete, inaccurate, coincidental, or unverifiable. VAERS reports often lack contextual information, such as total vaccinations given or information on unvaccinated groups for comparison. Most reports to VAERS are voluntary, which means they may be subject to biases. Data from VAERS reports should always be interpreted with these limitations in mind.”
In addition, COVID-19 vaccines were administered under emergency use authorization (EUA), not approval, which means they are subject to special VAERS requirements, as Health Feedback explained in an earlier review.
For approved vaccines, VAERS only requires healthcare providers to report certain adverse events of special interest that have been or might be potentially associated with the vaccine. But for vaccines under EUA, healthcare providers must report any serious adverse events that occur following vaccination “regardless of causality”. These include congenital disabilities and any adverse events that are life-threatening, involve hospitalization or increase its length, or cause a “substantial disruption of the ability to conduct normal life”. VAERS also requires healthcare providers to report any cases of myocarditis, pericarditis, multisystem inflammatory system, and COVID-19 cases that result in hospitalization or death.
The specific requirements for vaccines under EUA introduces a reporting bias towards increased reporting of serious adverse events among people who received a COVID-19 vaccine, making it impossible to draw conclusions about the number of adverse events for COVID-19 vaccines compared with any approved vaccine.
Claim 3 (Unsupported):
“I know in my own personal circle, though, plenty of people that had adverse events to this vaccine”
Toward the end of the video, Kirk mentioned “a lot of unfortunate things” that happened to people he knows, without providing any evidence that supports this claim. Specifically, he mentioned people who had been “paralyzed for the waist-down”, had heart issues, or “dropped dead” after receiving the vaccine.
Anecdotes, such as a person’s own personal experience can be influenced by many factors other than vaccination. Attributing an adverse event to something remarkable that happened shortly before is appealing but incorrect, as a STAT News article illustrated:
“Heart attacks occur most commonly in the morning, yet we don’t blame breakfast for causing them. A heart attack on the morning after a Covid-19 vaccine, though? That might be another matter.”
Furthermore, such cases are often unverifiable. These issues make anecdotes and testimonials unreliable to make assumptions about what caused an adverse event, unless there is scientific data to back them up.
Claim 4 (Incorrect):
“I don’t need to go vaccinate other people to prevent me of getting something the vaccine is supposed to prevent”
The widespread claim that choosing not to vaccinate only affects the person making the decision is incorrect. As Health Feedback explained before, a person’s decision not to vaccinate has consequences for the people surrounding that person. Although vaccine protection against infection and transmission is less than that against severe disease, research suggests that an unvaccinated person is still more likely to become infected or seriously ill and transmit the infection to others[9].
In contrast, a vaccinated person is less likely to become infected and develop severe disease, helping protect other people within the community, particularly those who are immunodeficient or can’t receive the vaccine for medical reasons. However, Kirk seemed to question the utility of a vaccine that can’t prevent 100% of infections. This misleading argument is known as the nirvana fallacy, which consists in dismissing a solution because it is imperfect, even if no perfect solution exists.
No vaccine is 100% effective. But it’s important to keep in mind that they don’t need to be to provide a public health benefit, as Health Feedback mentioned in earlier reviews. In an article for The Conversation, immunologist Sarah Caddy explained that even vaccines that don’t prevent infection have proven useful at reducing virus spread through the community by reducing the level of disease in the infected individual.
Although not perfect, the three COVID-19 vaccines authorized by the U.S. Food and Drug Administration (FDA) are highly effective against severe disease and death, which is the primary goal of a vaccine.
Conclusion
The arguments that Kirk provides in the video for opposing COVID-19 vaccines are based on anecdotes and misused safety data that don’t support his claims and actually contradict currently available scientific evidence. Rigorous analyses of safety monitoring data show that COVID-19 vaccines have a high safety profile and serious adverse reactions following vaccination are rare.


